2017 - Competency KM-A
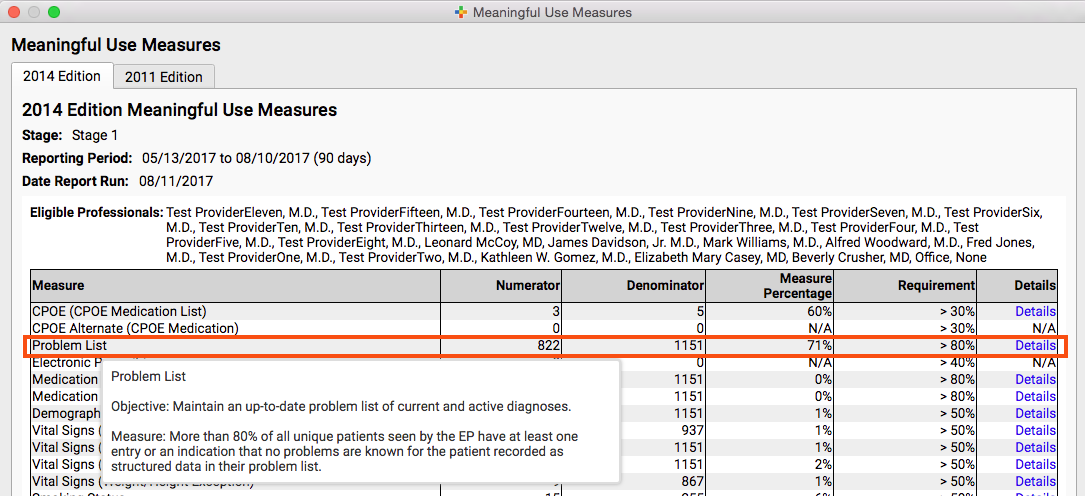
KM 01 (Core): Documents an up-to-date problem list for each patient with current and active diagnoses
| Description | Example/Screenshot/Documentation | Source | Date Added |
|---|---|---|---|
| Use PCC MU Report “Stage 1 - Problem List” | MU Report Example - Problem List | PCC | 8/10/17 |
{kind=link}
KM 02 (Core): Comprehensive health assessment includes (all items required):
- A. Medical history of patient and family.
Collects patient and family medical history (e.g., history of chronic disease or event [e.g., diabetes, cancer, surgery, hypertension]) for patient and “first-degree” relatives (i.e., who share about 50% of their genes with a specific family member).
- B. Mental health/substance use history of patient and family.
Collects patient and family behavioral health history (e.g., schizophrenia, stress, alcohol, prescription drug abuse, illegal drug use, maternal depression).
- C. Family/social/cultural characteristics.
Evaluates social and cultural needs, preferences, strengths and limitations. Examples include family/household structure, support systems, and patient/family concerns. Broad consideration should be given to a variety of characteristics (e.g., education level, marital status, unemployment, social support, assigned responsibilities).
- D. Communication needs.
Identifies whether a patient has specific communication requirements due to hearing, vision or cognition issues.
- E. Behaviors affecting health.
Assesses risky and unhealthy behaviors that go beyond physical activity, alcohol consumption and smoking status and may include nutrition, oral health, dental care, risky sexual behavior and secondhand smoke exposure.
- F. Social functioning.
Assesses a patient’s ability to interact with other people in everyday social tasks and to maintain an adequate social life. May include isolation, declining cognition, social anxiety, interpersonal relationships, activities of independent living, social interactions and so on.
- G. Social determinants of health.
Collects information on social determinants of health: conditions in a patient’s environment that affect a wide range of health, functioning and quality-of-life outcomes and risks. Examples include availability of resources to meet daily needs; access to educational, economic and job opportunities; public safety, social support; social norms and attitudes; food and housing insecurities; household/environmental risk factors; exposure to crime, violence and social disorder; socioeconomic conditions; residential segregation (Healthy People 2020).
- H. Developmental screening using a standardized tool. (NA for practices with no pediatric population under 30 months of age.)
For newborns through 3 years of age, uses a standardized tool for periodic developmental screening. If there are no established risk factors or parental concerns, screens are done by 24 months.
- I. Advance care planning. (NA for pediatric practices.)
As a pediatric practice, you get credit for this component and can claim "N/A"
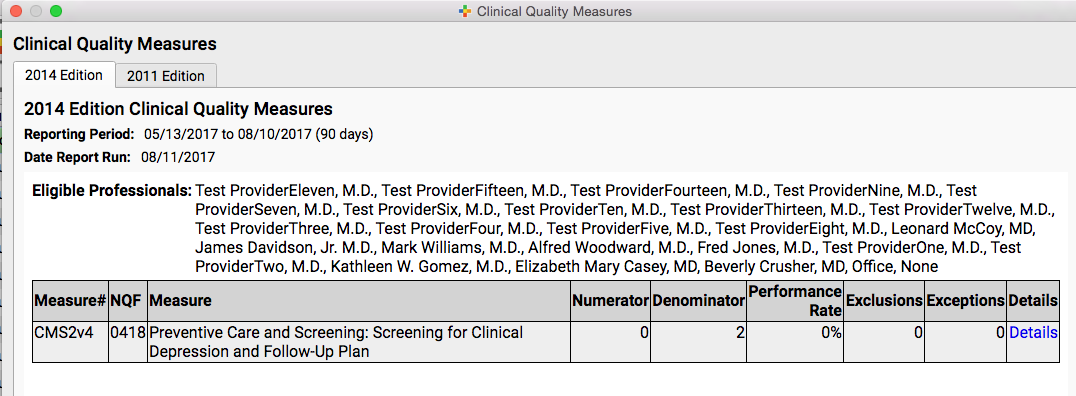
KM 03 (Core): Conducts depression screenings for adults and adolescents using a standardized tool
The documented process includes the practice’s screening process and approach to follow-up for positive screens. The practice reports screening rate and identifies the standardized screening tool.
| Description | Example/Screenshot/Documentation | Source | Date Added |
|---|---|---|---|
| Use PCC CQM Report “Screening for Clinical Depression and Follow-Up Plan” | CQM Report Example | PCC | 8/11/17 |
{kind=link}
KM 04 (1 Credit): Conducts behavioral health screenings and/or assessments using a standardized tool. (Implement two or more.)
View the AAP's list of mental health screening and assessment tools
- A. Anxiety.
The practice conducts screening for the presence of emotional distress and symptoms of anxiety using any validated tool (e.g., GAD-2, GAD-7).
- B. Alcohol use disorder.
The American Academy of Pediatrics’ (AAP) Bright Futures recommends clinicians screen all adolescents for alcohol and drug use during all appropriate acute care visits using developmentally appropriate screening tools. (e.g., CRAFFT or Alcohol Screening and Brief Intervention for Youth).
- C. Substance use disorder.
Available screening tools may include the Screening, Brief Intervention and Referral to Treatment (SBIRT) tool, CAGE AID or DAST-10 instruments which assess a variety of substance use conditions.
- D. Pediatric behavioral health screening.
This may include tools such as the Behavioral Assessment System for Children (BASC).
- E. Post-traumatic stress disorder.
- F. Attention deficit/hyperactivity disorder.
The Vanderbilt Assessment Scale or the DSM V ADHD checklist for adults or children/adolescents are examples of screening tools used to determine if a patient has Attention Deficit/ Hyperactivity Disorder (ADHD).
- G. Postpartum depression.
The AAP’s Bright Futures acknowledges that primary care practices that see both infants and their families have a unique opportunity to integrate postpartum depression screening into the well-child care schedule. Validated screening tools may include PHQ-2, PHQ-9 or Edinburgh Postnatal Depression Scale (EPDS) or other validated screening tools, and may be conducted 4–6 weeks postpartum or during the 1-, 2-, 4- or 6-month well-child visits.
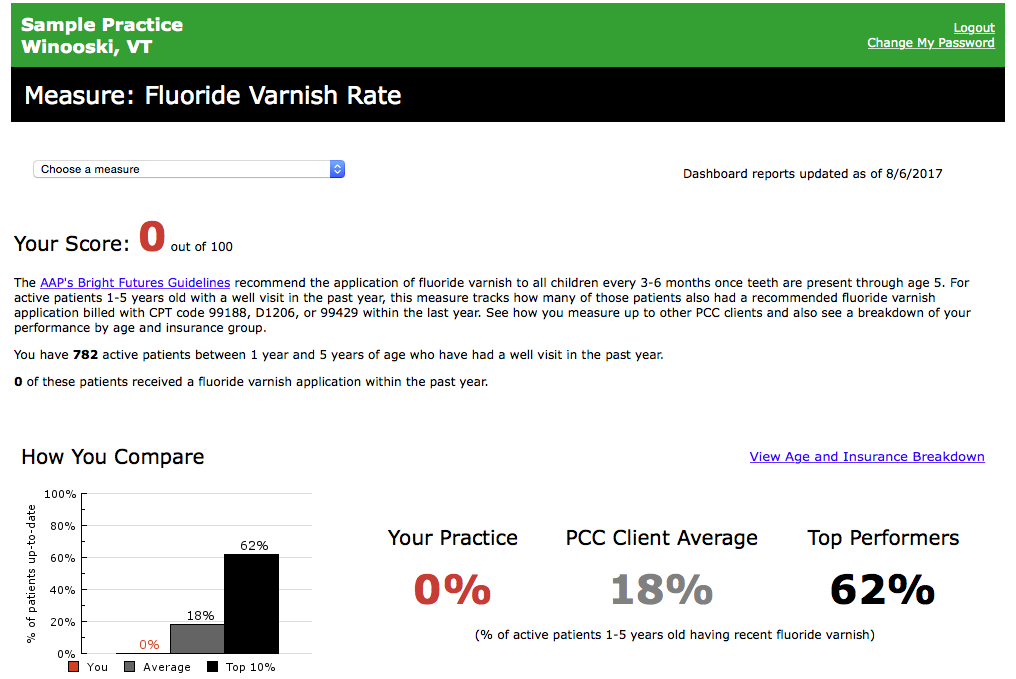
KM 05 (1 Credit): Assesses oral health needs and provides necessary services during the care visit based on evidence-based guidelines or coordinates with oral health partners
The practice conducts patient-specific oral health risk assessments and keeps a list of oral health partners such as dentists, endodontists, oral surgeons and/or periodontists from which to refer.
| Description | Example/Screenshot/Documentation | Source | Date Added |
|---|---|---|---|
| Monitor Fluoride Varnish rate measure in Dashboard | Dashboard Fluoride Varnish Rate Example | PCC | 8/11/17 |
{kind=link}